
How the Prior Auth Deadline Is Affecting Vendors Who Don't Sell Prior Auth
Health plans met the deadline by speeding up denials. Now they have problems in appeals, provider relations, and member experience.

Upward Growth provides health tech leaders with the playbooks and proof to transform complex markets into real growth. Each week, we deliver clear, practical strategies on positioning, messaging, and growth, so leaders can close enterprise deals and build repeatable momentum.
🤝 Work with Ryan on payor growth strategy: Contact me
🟦 Connect with the author, Ryan Peterson, on LinkedIn.
💡 Newsletter sponsorships are available: Learn More
Three regulatory deadlines are reshaping how health plans operate, what they prioritize, and how much bandwidth they have for new vendor relationships. If you’re selling to health plans, these deadlines are already affecting your pipeline, whether anyone told you or not. If you work at a health plan, you’re living this, and your vendor partners need to understand what you’re dealing with.
At the end of last year, I published “Five Trends That Will Shape Health Tech Sales Cycles in 2026.” Prior authorization compliance was one of them, and I’m going deeper on it here because understanding the regulatory timeline helps you understand your buyers.
Here’s what’s unfolding:
January 1, 2026 (just passed): Operational requirements went live. Plans must now respond to expedited prior auth requests within 72 hours and standard requests within seven days. They must provide specific denial reasons. And they had to hit these requirements manually, without the technology infrastructure to support them.
March 31, 2026 (two months away): Public reporting begins. Every impacted plan must post its prior authorization metrics on its website. Denial rates, approval rates, turnaround times, and appeals outcomes become visible and comparable for the first time. Plans with poor numbers will face questions from brokers, consultants, and members.
January 1, 2027: Technology requirements take effect. The FHIR-based APIs that would have made the operational changes sustainable finally arrive, a full year after plans needed them. This will trigger another wave of implementation work.
This isn’t a single compliance moment but a two-year wave that’s already affecting health plan buying decisions and will continue to do so through 2027.
If your health plan deals slowed in the back half of 2025, this is probably why. If you’ve been waiting for the right moment to re-engage, the window between the January deadline and March reporting is it. This article breaks down what changed, what problems compliance created for plans, and how vendors outside the prior auth space can position themselves around it.
What January 1 Actually Required (And What It Didn’t)
The CMS Interoperability and Prior Authorization Final Rule created two sets of requirements with different deadlines. The technology requirements, specifically the FHIR-based APIs for electronic prior authorization, don’t take effect until January 1, 2027. Most of the industry conversation focused there.
But the operational requirements went live on January 1, 2026. If you've noticed health plan buyers being harder to reach or pushing timelines, this is partly why.
Decision timelines got compressed. Medicare Advantage plans, Medicaid MCOs, CHIP, and ACA exchange plans must now respond to expedited prior authorization requests within 72 hours and to standard prior authorization requests within 7 calendar days. For plans already operating at two to three-day turnarounds, this changed almost nothing. For plans that were routinely taking ten to fourteen days, it required a fundamental operational overhaul.
Denial reasons must be specific. Plans can no longer issue vague denials. They must provide specific reasons, regardless of whether the request was submitted by fax, portal, or phone. This sounds minor, but it means UM teams now need to document clinical rationale for every denial in a way that can be communicated back to providers. That’s new work.
Metrics collection started. Plans must now track and collect prior authorization data that will be publicly reported by March 31, 2026. Denial rates, approval rates, turnaround times, and appeals outcomes will become visible and comparable for the first time.
Not all plans are equally affected. Plans that already operated with tight turnarounds experienced minimal disruption, often because state requirements were already more aggressive than federal standards. These plans made minor adjustments and moved on. Plans that had been operating at the slower end of the range had to overhaul their UM operations without the technology to support them. They added staff, created workarounds, and are now running on manual processes that won’t scale.
If you’re selling into health plans, understanding where your target accounts fall on this spectrum tells you whether they have bandwidth for new initiatives or whether they’re still buried in compliance work.
Faster Denials, More Appeals, Angrier Providers
The new prior auth requirements forced plans to respond faster. Many responded by denying faster. That's creating problems in appeals, provider relationships, and member experience (all problems that have nothing to do with prior auth solutions).
The fastest way to hit a 72-hour or seven-day turnaround isn’t to make better decisions faster. It’s simply to make faster decisions. For some plans, that meant issuing denials more quickly rather than taking the time to work with providers on documentation or alternative approaches.
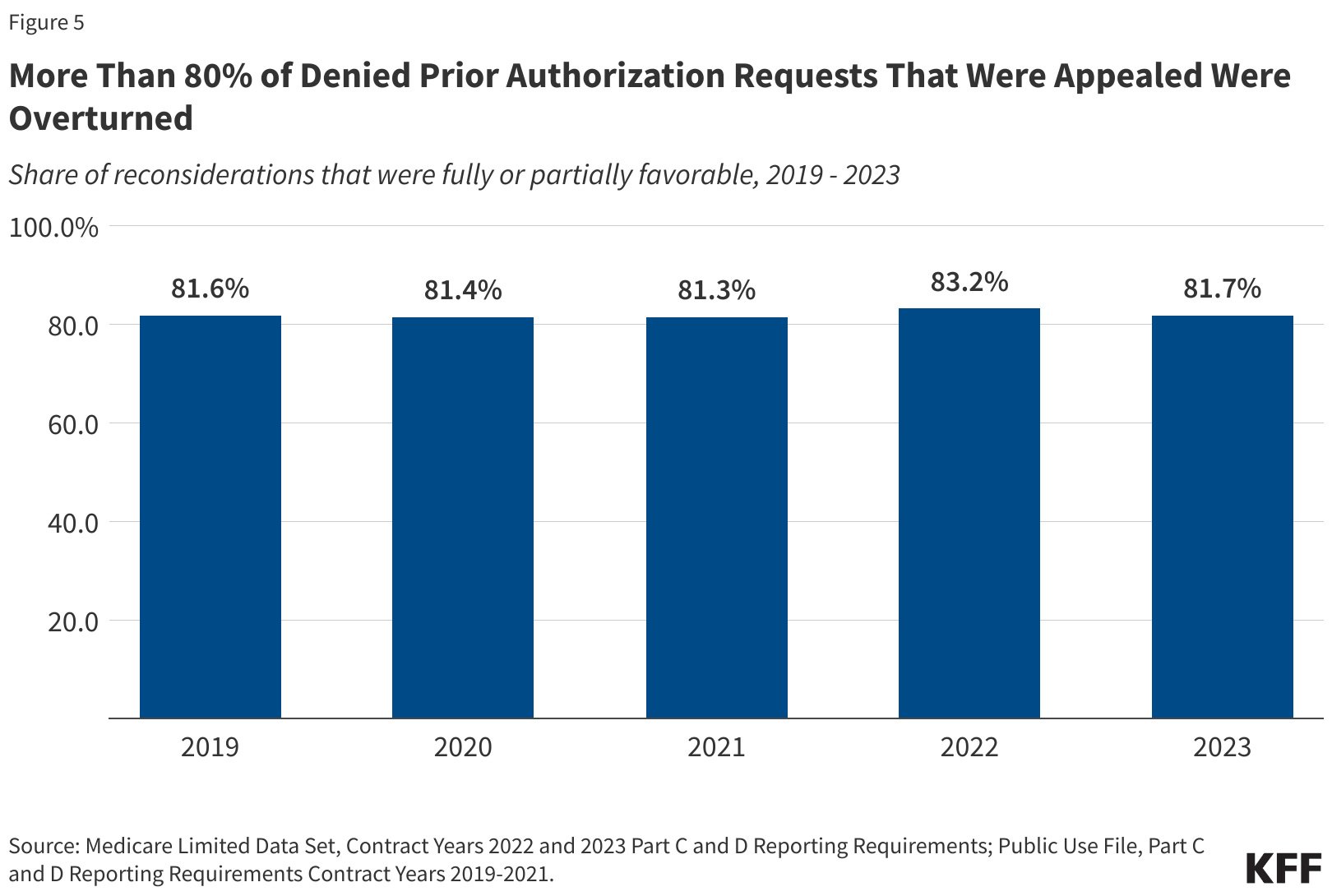
And the math is stark. MA plans processed nearly 50 million prior authorization requests in 2023, with about 6.4% denied. But among denials that were appealed, 82% were overturned. That’s not a rounding error. It’s a signal that a significant share of initial denials shouldn’t have been denials at all.
Now compress the decision timeline without changing the underlying review process. You get the same dynamic, just faster. More denials issued quickly. More appeals filed. More provider frustration. More member friction.
You can quickly see how this spirals and creates downstream problems that have nothing to do with prior authorization technology:
Provider abrasion increases. Physicians report spending an average of 13 hours per week on prior authorizations, completing roughly 39 requests per physician per week. When denials come back faster but don’t improve, provider relationships are going to suffer. This will show up in network satisfaction scores, willingness to participate in value-based arrangements, and the plan’s ability to maintain competitive networks.
Member experience takes a hit. When members experience delays or denials, their perception of the plan suffers. This happens to more than half of insured adults who need specialized care. For MA plans, member perception directly impacts CAHPS scores, which feed into Star Ratings. A plan that “solved” prior auth compliance by denying faster may have created a member experience problem that costs them more in quality bonus revenue than they saved in medical expense.
Appeals volume grows. Faster denials with specific denial reasons (now required) make it easier for providers and members to understand why something was denied and to file an appeal. Plans that weren’t staffed for increased appeals volume are now dealing with backlogs.
This is about to get worse. Providers are increasingly using AI tools to automatically generate appeals, and some can fire off an appeal within hours of receiving a denial. Plans are responding with their own AI to process the volume. The result is an escalating automation arms race that will drive appeal volume even higher and create more pressure on the staff, systems, and processes that support it.
Prior auth compliance didn't eliminate friction. It relocated it. Plans that met the deadline by speeding up denials now have problems in appeals, provider relations, and member experience. Those are problems that vendors outside the prior auth space can help solve.
Prior auth compliance didn't eliminate friction. It relocated it.
The March Reporting Deadline Is Your Sales Lever
The public reporting requirement changes the sales conversation for any vendor who can credibly claim they improve the metrics that are about to become visible.
By March 31, 2026, every impacted payer must post prior authorization metrics on their public website: denial rates, approval rates, average and median turnaround times, and appeals outcomes. For the first time, these numbers will be visible to brokers selecting plans for employer groups, consultants advising on network decisions, and members comparing options during open enrollment.
Plans with poor metrics will face questions they’ve never had to answer before. Why is your denial rate 15% when the plan down the street is at 8%? Why do 40% of your denials get overturned on appeal? These aren’t hypothetical concerns. They’re competitive differentiators that will influence enrollment and retention.
If your solution can credibly improve the metrics that plans are about to publicly report, you have a window right now where that message lands differently than it did six months ago.
The positioning isn’t complicated: Your March 2026 numbers are going to be public. What’s your plan to make them defensible?
That question opens doors for vendors across categories:
Member engagement vendors can reduce the friction that leads to complaints and disenrollment.
Care management vendors can improve care coordination and reduce the need for prior auth in the first place.
Provider engagement solutions can reduce documentation deficiencies and first-pass denial rates.
Appeals management vendors can improve initial decision quality.
The key is connecting your solution to the specific metrics that will be visible. Vague claims about “improving member experience” won’t land. Specific claims tied to denial rates, turnaround times, or appeals outcomes will.
How This Changes Your Approach
If you're selling member engagement, care management, provider engagement, analytics, or anything else that isn't prior auth technology, the last six months probably felt like pushing uphill. Deals that were moving stopped moving, and you may not have heard "prior auth" as the reason (but it was likely the cause). Health plans were consumed by the operational changes they had to implement manually, and, as a result, many other initiatives were deprioritized.
That’s starting to shift as the January deadline has passed. Plans are through the worst of the operational scramble. But they’re not out of the woods yet. The way many of them met the March deadline has created new problems: appeals backlogs, provider friction, and member experience hits. And in two months, their metrics will go public for the first time.
This is a different selling environment than six months ago. Bandwidth is returning. The problems compliance created are exactly the problems that member engagement, care management, and provider engagement solutions can solve. And March 31 gives you a concrete reason to reach back out: plans are about to be publicly accountable for metrics your solution can improve.
If you’ve been waiting for the right moment to re-engage your health plan accounts, this is it. The window between “through the crisis” and “moved on to the next thing” doesn’t stay open long.

You’ve reached the end of the free article.
Everything above is the landscape: what changed, what problems it created, and why the next 60 days matter. What’s below is what I actually use with clients: positioning scripts for the “compliance created new problems” conversation and how to use March reporting pressure as a sales lever without overselling it.
Paid subscribers get this section plus the full archive of frameworks, scripts, and deep-dives.